COVID-19’s Impact On Healthcare Design
FCA
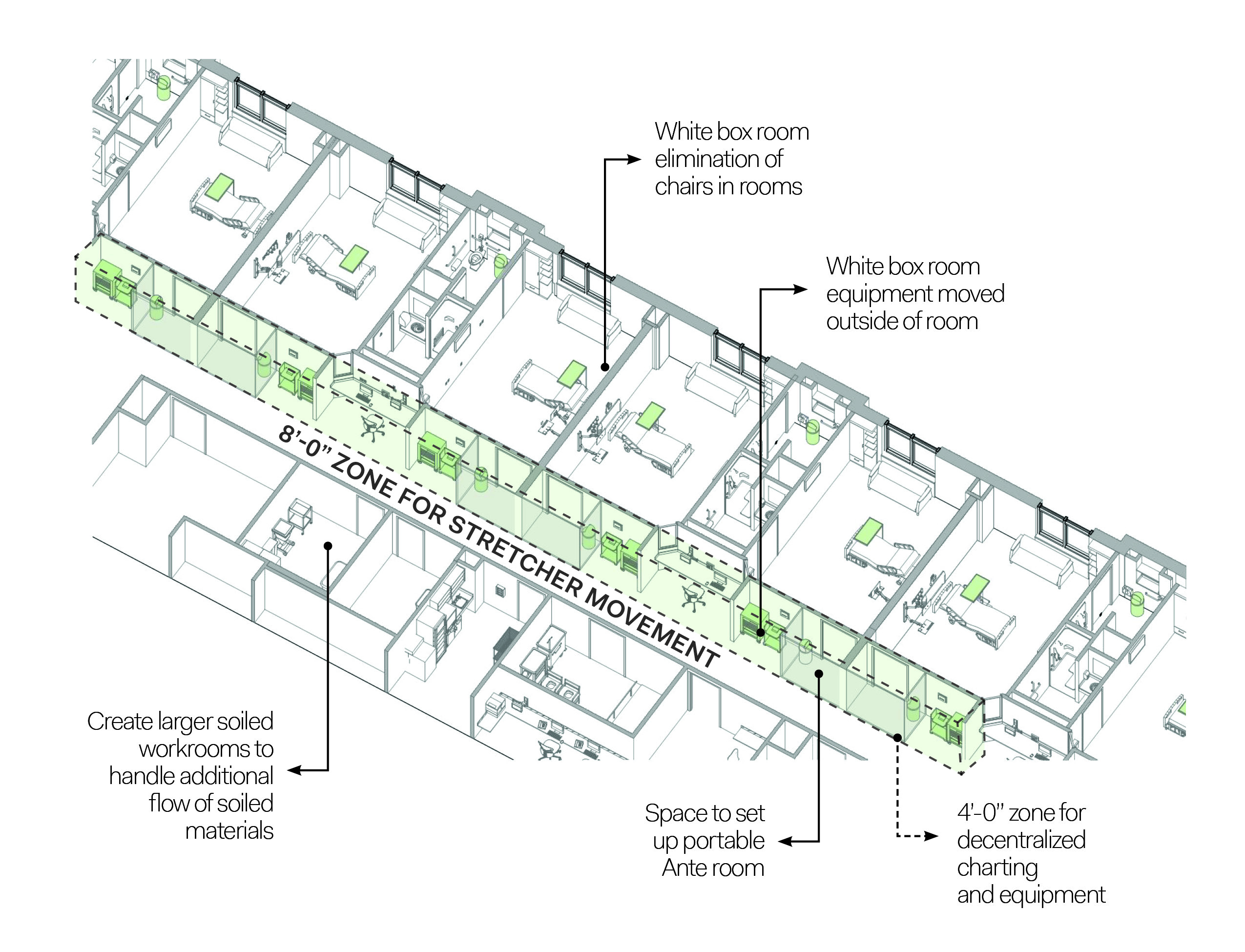
A flexible, acuity-adaptable patient care unit is designed with wider hallways that accommodate temporary ante rooms and equipment.
How did COVID-19 affect the healthcare industry?
Seeking to gain a deeper understanding of what the healthcare industry was facing throughout the COVID-19 pandemic and the key design issues associated with the challenges faced, FCA conducted a series of client interviews.
This series of interviews took place over a five-month period with 15 key stakeholders from six Northeast healthcare institutions, both urban and suburban, to understand the major takeaways and overall impact of COVID-19 on the healthcare industry.
A list of standardized questions on patient care delivery, public interaction, staff fatigue, medical equipment, and indoor air quality were utilized in virtual interviews with senior administrators, clinicians, nurses, facility teams, and support services staff.
Overall, these interviews showed that healthcare facilities were largely unprepared for the COVID-19 pandemic and faced incredible obstacles over these past two years as a result. Hospitals and healthcare systems alike are now taking a deep look into what changes can be made from both an operations standpoint and a design perspective to better prepare for future widespread illnesses.
Below are some of the key findings.
Patient care delivery
Looking at patient care delivery, the survey focused on three basic areas: patient treatment, use of spaces, and cleaning protocols.
We identified a set of key findings relating to patient care that include minimized patient interaction, a lack of equity between facilities, changing standards for care delivery, patient visualization, and the increased use of temporary surge units.
Many locations reported that they minimized staff and patient interaction during surges. While this didn’t come as a surprise, what’s interesting to note is the way that facilities uniquely navigated these challenges, especially as it pertains to patient care. In existing medical/surgical bed units, a number of temporary ante rooms were constructed and wall sleeves were installed between corridor and patient rooms to allow equipment to be controlled from hallways.
Also, most interviewees noted they had utilized temporary surge units. The space types varied from repurposed perioperative recovery areas to retrofitted behavioral units, ORs, and other medical/surgical units. Medical gases and temporary exhaust ventilation were added to support patient care in these temporary treatment spaces.
Patient and visitor screening
Facility team respondents relayed how their creativity and resources helped problem-solve during the height of the first wave and how this experience will impact design and planning of future projects. Solutions ranged from screening at entry points to ways of improving airflow into ICU rooms.
At the onset of the pandemic, screening everyone who entered the facilities was paramount, and with limited knowledge of COVID-19, the fastest and simplest diagnostic measure was monitoring for fevers. Technology was used to register temperature, quickly identifying any possible infections.
Facilities quickly installed power and data that was needed at entries to implement remote thermal scanning and temperature guns, which continue to be used in hospital settings and have also been rolled out across outpatient settings.
Healthcare staff fatigue
Healthcare staff continue to be affected by COVID-19, as they face staffing issues, not only from within the hospital system, but at a global scale. Prior to the pandemic, the healthcare industry as a whole was facing staffing shortfalls of both nurses and physicians according to the American Nurses Association and the American Hospital Association.
Staff burnout, anxiety, mental health, loss of respect, and trust from the general public are all noted as reasons why people are leaving the healthcare workforce.
Respondents also noted that staff have felt anxiety about keeping their families safe at home. Inpatient units typically do not have locations set aside for staff to don and doff PPE garments. Rooms were designated for this to take place; however, staff still didn’t feel comfortable going home in clothing that had been within the hospital. Many were changing in their cars or garages to keep their homes and families safe from infection.
This was especially true during the first year of the pandemic, but as more is known about the disease and more vaccinations are available, the anxiety of this has decreased.
Medical equipment & COVID
Ventilators were stored in case of another surge, while Bi-pap and CPAP were actively being used to keep people off ventilators. This type of equipment presents ongoing challenges for staff as cleaning and storage processes must continuously be revisited.
Hospitals got creative about using spaces that weren’t designed for critical care patients, such as waiting areas and conference rooms. They had to quickly change the standards of care delivery, based on what resources (space, staff, equipment) were available on a day-to-day basis.
Higher patient acuity required direct observation and staff found communication to be difficult due to the existing interior architecture of the unit which wasn’t designed for high-acuity patients.
An increased presence of technology across numerous facilities helped to resolve some of the communication and visualization challenges. Clinical teams got creative with the resources available and used baby monitors to keep an eye on patients while attending to other patients’ needs. Today, those baby monitors are being replaced with cameras that are specially designed for healthcare environments.
Adaptable healthcare spaces
Dedicating units into COVID-19 units was the biggest change hospitals faced. Engineers, contractors, architects, and facilities teams worked together to fabricate ways to update patient rooms. Converted units underwent changes to doors, electrical requirements, and air exchange increases.
Changes to solid doors were a staff and patient safety issue, as being able to see into the room from the corridor was critical with this highly infectious disease.
In a typical medical/surgical unit, charting is done at a central location, but with ICU patients, direct observation is needed, and staff found themselves sitting in corridors with computers. Power and data were added at locations outside rooms so that this adjacency could be maintained.
Hospital indoor air quality
Interviewees stated that initially it was thought that indoor air in patient rooms would require not only outside air but also HEPA filtration systems. Many stated that curtain wall systems were retrofitted with HEPA filtration systems. After more was learned about how the virus spreads, these rooms were changed to full exhaust with additional air exchanges in patient rooms.
Survey participants stated that most filtration systems had to be upgraded and were not capable of handling the amount of air exchanges required as well as increased direct exhaust. Most hospital buildings are designed without operable windows, so providing fresh air proved to be challenging to accommodate the ventilation and direct exhaust required.
New projects that are being planned are considering operable windows and including higher levels of air.
Future-proofing design strategies
The pandemic has changed both healthcare delivery and how facilities are designed. As more project teams look for design elements for future proofing of surge and pandemic-capable spaces, here are some considerations.
1. Plan for large population health events
As hospitals continue to address surges of COVID-19 patients and evolving knowledge about the pandemic and variants becomes available, they’re gaining an understanding of what it takes to accommodate large population health events. This isn’t going away and new large population health events will occur.
Consideration of architectural solutions such as larger lobby entry queuing sequences that allow for safe temperature scanning and entering a facility are necessary.
Separating out staff entry sequences is also a way to accommodate the public more easily than mixing staff in with them during pandemic surges. Exterior panelized walls and modular infrastructure systems can be added to building exteriors to expand and contract entrance sequences, allowing patients to wait within temperate space.
Current waiting areas should be modified and future waiting areas should be designed to meet safe distance separations requirements of six feet, with furniture quantities reduced and seating areas should be arranged in smaller groupings to maintain distancing.
2. Flexible and adaptable is the new normal
Developing patient rooms that can flex to different acuity levels was once considered a luxury but now it’s a must-have. These flexible units are designed to the highest level of critical care with higher medical gases, more air changes and direct exhaust, higher power supply all to meet the critical care requirement.
The design of these flexible units should consider the additional equipment needs that ventilators and bi-pap units bring to the design, and patient rooms should be sized to accommodate this equipment at the critical care level.
Wider hallways should be considered within these units to 12’-0” to accommodate temporary ante rooms and additional equipment staging. This comes with added costs, and hospitals are weighing the pros and cons of how many of these types of units to build.
3. Staff safety
Staff are a precious resource. One way to keep them safe is to provide the proper PPE supplies during population health events. Hospitals are re-evaluating the amount of storage needed and identifying the appropriate levels of PPE to keep on hand for use during surges.
Designers can help institutions look for underutilized spaces within the hospital campus to help store supplies. Additional support spaces should be considered to allow staff to transition from infectious spaces to clean areas, take off PPE, shower, and change into non-infected clothing to travel home.
Providing two sets of doors that are normally kept open but can be shut to create an ante room space for PPE donning/doffing is another way to aid in keeping staff safe and provide ease of PPE use.
4. Leverage technology
Better communication can help patients understand the proposed treatments, and a caregiver can be part of those discussions. Using voice-activated devices in the rooms can allow nursing teams to accomplish tasks remotely. Technology can be leveraged to give patients who are able control of certain elements such as window shades, lighting, temperature, and ordering food.
Early in the pandemic and even now, hospitals are using artificial intelligence combined with imaging and clinical data to analyze which patients had coronavirus disease (COVID-19). Additionally, technology such as tablets and video conferencing capabilities in patient rooms can keep families and patients connected
5. Building better infrastructure
Without the right building systems in place to support patient care, the availability of space doesn’t matter. Hospitals are now considering including the costs of building increased power, medical gases, fresh air, and direct exhaust infrastructure to accommodate for adaptable spaces for pandemic use.
And having a plan in place through the design of adaptable patient care units along with the infrastructure resources on reserve for these events can help make patient care during a pandemic more manageable. Older infrastructure should be considered for update/replacement to accommodate the air quality that is required for infectious patients.
Future of healthcare design
In this evolving landscape, healthcare designers need to stay on the forefront of changes to combat this pandemic and the next. Future proofing and developing flexible, adaptable spaces are the best ways we can help healthcare institutions.
Catherine Gow, AIA, NCARB, Lean Six Sigma, is principal, health facilities planning at FCA (New York). She can be reached at cgow@fcarchitects.com. Jennifer Kenson, CHID, IIDA, NCIDQ, ASID, is principal, interior design at FCA (Philadelphia). She can be reached at jkenson@fcarchitects.com.

